CAPSIDA APPROACH
Capsida Biotherapeutics is a fully integrated next-generation genetic medicine company. Capsida’s approach unlocks the potential to treat both rare and common neurologic and ocular diseases across all ages.
Central Nervous System (CNS)
We are advancing intravenously (IV) delivered gene therapies for the CNS that have broad, brain-wide neuronal expression.
OPHTHALMOLOGY
For diseases of the eye, Capsida is directing its platform to engineer capsids for local intravitreal (IVT) and suprachoroidal (SCS) delivery.
CAPSID ENGINEERING AND PRECLINICAL
At Capsida, the scale at which we have engineered capsids is unrivaled. Using our automated, high-throughput biological screening, our scientists assess large, diverse engineered capsid libraries for CNS and the eye in models relevant to humans to quickly identify optimal capsids that target tissues and cells in organs of interest.
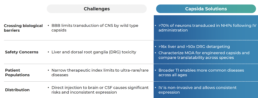
We have developed engineered capsids for the brain that transduce >70% of neurons brainwide, generating a significantly increased therapeutic index. We have identified novel human blood-brain barrier receptors that bind our engineered capsids and are conserved between primates and humans. Our therapies can deliver a broad range of cargos including gene replacement, gene editing, gene silencing and vectorized antibodies, among others.
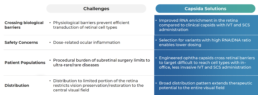
Capsida’s engineered capsids for ocular diseases have improved RNA enrichment in the retina compared to clinical capsids while utilizing less invasive IVT and SCS dosing.
MANUFACTURING OPERATIONS
Capsida’s manufacturing operations have successfully supported two IND packages. We have built capabilities based on a HEK 293 platform to perform all process development and analytical activities in-house to enable rapid transition from pre-clinical to clinical studies while controlling quality, costs, and timelines. We have implemented field-leading process and analytical capabilities including transitioning from three-plasmid to two-plasmid system and developing product specific potency assays and an extensive internal assay panel. This eliminates the need and the cost of contract development and manufacturing organizations (CDMOs). We initiate manufacturability assessments early in the capsid engineering process to ensure high product quality and productivity. We have built a state-of-the-art cGMP manufacturing suite. Our industry leading yields demonstrate consistent performance from 2L to 50L to 200L cGMP scale.
EPILEPTIC ENCEPHALOPATHIES (STXBP1)

Syntaxin-binding protein 1 (STXBP1) encephalopathy is a devastating neurodevelopmental disorder affecting nearly one in 30,000 children. It is associated with severe developmental delay, treatment-resistant seizures, and early death.
STXBP1 encephalopathy is caused by mutations in the STXBP1 gene encoding a protein involved in the release of neurotransmitters and neuropeptides, which are responsible for communication across neurons in the brain and central nervous system.
There are no specific therapies for STXBP1 encephalopathy today. Treatment is supportive and includes anti-seizure medication and physical, occupational, and speech therapy to somewhat lessen the impact on daily life for patients and their families.
Capsida is developing a novel gene therapy, , for the treatment of this severe diseaseOur program is designed to stably replace STXBP1 protein throughout the brain after a single intravenous infusion, with the hope of correcting underlying pathology and significantly improving symptoms and quality of life for children with STXBP1 encephalopathy. [link to advocacy site (URL NEEDED)]
López-Rivera et al, 2020, Abramov et al, 2020, Stamberger et al, 2016, Saitsu et al., 2008; Stamberger et al., 2016
GBA-1 PARKINSON’S DISEASE

Parkinson’s disease is a brain disorder that causes unintended or uncontrollable movements, such as shaking, stiffness, and difficulty with balance and coordination. Symptoms usually begin gradually and worsen over time. As the disease progresses, people may have difficulty walking and talking. They may also have mental and behavioral changes, sleep problems, depression, memory difficulties, and fatigue.Mutations in GBA1, which encodes lysosomal enzyme glucocerebrosidase (GCase), are a relatively prevalent risk factor associated with Parkinson’s disease and aggravating disease progression. GBA1 mutations increase risk for developing PD (and related neurodegenerative disorders). PD-GBA similar to idiopathic PD, earlier onset and more rapid progression.
AMYOTROPHIC LATERAL SCLEROSIS (ALS)

Amyotrophic lateral sclerosis (ALS or Lou Gehrig’s disease) is a devastating, late-onset, neurodegenerative disease characterized by loss of both upper and lower motor neuron function. ALS affects approximately 6 in 100,000 individuals. While most cases are sporadic, familial ALS is observed in 5 to 10% of individuals who are diagnosed with ALS.
Clinically, ALS presents with focal muscle weakness, twitching or slurred speech, over time the symptoms intensify and spread to the whole body. Eventually, affected individuals lose the ability to move, chew, swallow, speak and breathe. On average, death occurs within 3 to 5 years of symptom onset.
There is no cure for ALS. Current treatments options have been shown to slow the progression of symptoms and improve quality of life but they can’t reverse the damage or stop the motor neuron demise occurring throughout the brain and spinal cord.
Capsida is developing novel gene therapy for the treatment of ALS. Delivered in a single intravenous infusion and designed to target both upper and lower motor neuron degeneration, our hope is to address the progressive loss of function and ultimately the loss of life in patients with ALS.
Mehta et al., 2018; Ajroud-Driss and Siddique 2014; ALS Association website: als.org
FRIEDREICH’S ATAXIA (FA)
Friedreich’s ataxia (FA) is a debilitating, life-shortening degenerative neuromuscular disorder affecting approximately 1 in 50,000 people. Typically, onset begins in childhood and adolescence and is characterized by progressive loss of balance and coordination and muscle weakness, leading to confinement to a wheelchair. Disease advancement is also associated speech, vision, and hearing impairment as well as heart conditions and diabetes.
Friedreich’s ataxia is caused by a defect in the frataxin gene (FXN) that leads to decreased levels of the protein frataxin. This deficiency leads to decrease cell energy production that results in the degeneration of nerve cells in the brain and spinal cord. There are no currently approved therapies to slow or reverse the disease and treatment is focused on symptom management including physical, occupational and speech therapy.
Capsida is developing a novel gene therapy for the treatment of FA. Delivered as a single intravenous infusion and targeting the underlying pathology, our aim is to alter the progression of disease and improve the quality and length of life of those affected by FA.
Zesiewicz et al; Burk et al 2017; Cook et al 2017; Zhang et al; Corben et al.